
The defining health challenge of 2026 is not weight loss; it is muscle preservation. While GLP-1 agonists (Semaglutide/Tirzepatide) effectively reduce mass, up to 40% of that loss is lean tissue. The solution is a synergistic protocol combining Low-Energy Ketogenic Therapy (LEKT) to biochemically spare amino acids, and Corrective Strength Training to mechanically signal retention. At RxFit, we implement this “Asset Protection” strategy for Austin executives to prevent sarcopenic obesity.
Key Takeaways
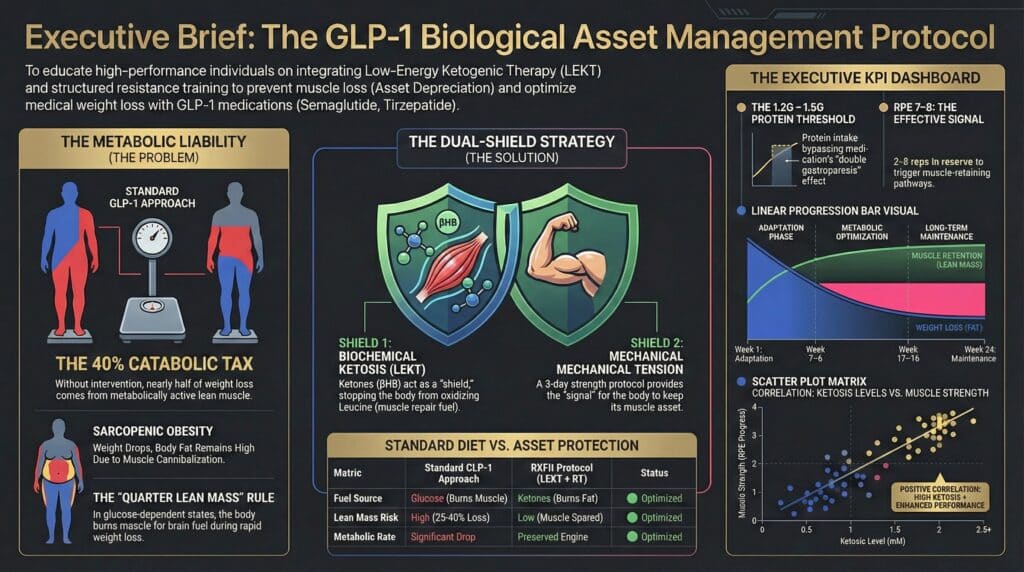
- Asset Protection: Without intervention, rapid GLP-1 weight loss liquidates your metabolic engine (skeletal muscle), slowing your resting metabolic rate.
- The Biochemical Shield: Beta-Hydroxybutyrate ($\beta$HB) inhibits the oxidation of leucine, effectively “locking” amino acids in the muscle tissue during a caloric deficit.
- Tension over Trauma: High-intensity cardio on a calorie-restricted body is catabolic. You need controlled, biomechanically precise strength training to signal growth.
- The RxFit Method: Led by Danny Trejo (Corrective Exercise Specialist) and Nini Maine (Functional Nutritionist), we combine clinical nutrition with corrective mechanics in Westlake and The Domain to ensure you lose fat, not function.
Why is my body “eating” muscle while on GLP-1s?
For the Industrial Athlete—the CEO in Westlake or the Founder in The Domain—the body is a capital asset. Taking a GLP-1 agonist without a preservation strategy is akin to selling off your most valuable machinery to pay the electricity bill. This is “Asset Depreciation.”
When you induce a profound caloric deficit using agents like Semaglutide, the body follows the “Quarter Lean Mass Rule.” Historically, 25% to 40% of weight lost is Fat-Free Mass (FFM). This occurs because, in a glucose-dependent state, the body breaks down skeletal muscle to convert amino acids (alanine and glutamine) into glucose for the brain via gluconeogenesis.
This leads to Sarcopenic Obesity: a condition where you weigh less, but your body fat percentage remains high because you have cannibalized your structural integrity. This lowers your Resting Metabolic Rate (RMR), creating a “metabolic trap” that makes weight regain inevitable once the medication stops. At RxFit, we view this muscle loss as a preventable liability to your long-term health portfolio.
How does Ketosis act as a “biochemical shield” for muscle?
At RxFit, we do not guess; we follow the physiology. The solution to catabolism is to change the fuel source. By shifting into Low-Energy Ketogenic Therapy (LEKT), we alter the body’s demand for glucose.
When your brain adapts to using ketones (acetoacetate and $\beta$-hydroxybutyrate) for fuel, the demand for glucose plummets. Consequently, the signal to break down muscle tissue for gluconeogenesis is attenuated.
Furthermore, the ketone body $\beta$HB acts as a powerful signaling molecule. Research indicates that $\beta$HB specifically inhibits the oxidation of leucine, the primary branched-chain amino acid responsible for muscle repair. It also suppresses the NLRP3 inflammasome, reducing the systemic inflammation that drives muscle wasting.
Recent 2025 data from the Schiavo study confirms this: Patients on Tirzepatide combined with a ketogenic protocol retained significantly more muscle mass and strength than those on a standard low-calorie diet. We use nutrition to biochemically “spare” the muscle, so we can train it.
Why is corrective strength training non-negotiable?
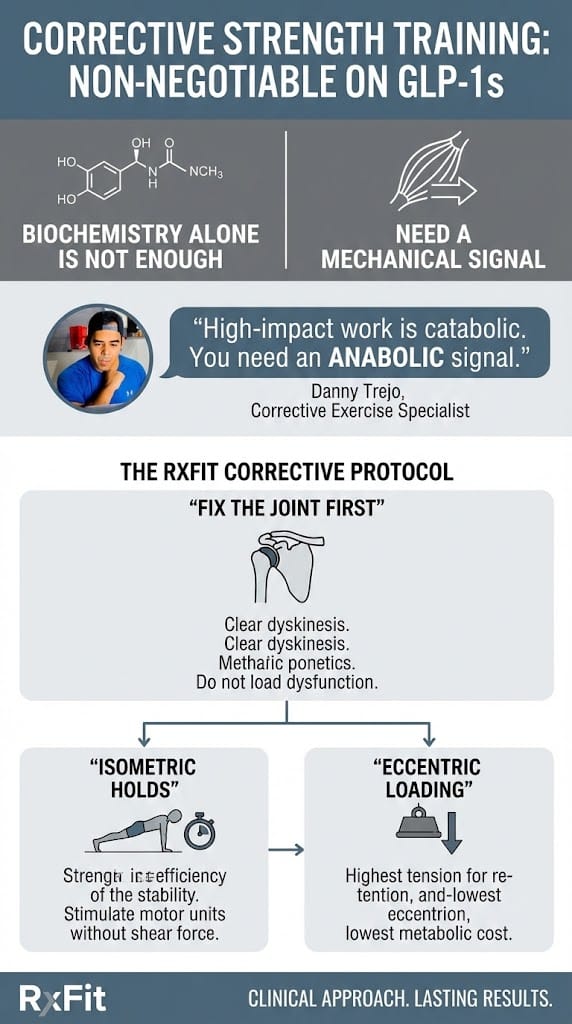
Biochemistry alone is not enough; you need a mechanical signal. However, training while on a GLP-1 agonist requires a specific clinical approach. You cannot simply “go to the gym” and perform random acts of fitness.
Danny Trejo, Corrective Exercise Specialist, warns against “burning calories” through high-impact cardio while on these medications. “When you are in a caloric deficit, your recovery capacity is compromised. High-impact work is catabolic—it breaks you down. You need an anabolic signal.”
We prioritize Hypertrophy through Stability. Because rapid weight loss shifts your center of gravity, your proprioception (body awareness) is altered. Loading a dysfunctional joint in this state leads to injury.
The RxFit Corrective Protocol:
- Fix the Joint First: We clear “Upper Crossed Syndrome” and scapular dyskinesis before overhead pressing. We do not load dysfunction.
- Isometric Holds: We use static contraction to stimulate motor units without shearing forces on the joints.
- Eccentric Loading: We focus on the lowering phase of the lift, which generates the highest mechanical tension for muscle retention with the lowest metabolic cost.
How does RxFit integrate Nutrition and Training?
Generic trainers tell you to “eat less and move more.” That is dangerous advice for a GLP-1 patient. We treat your body as a high-performance system requiring precise calibration.
The Nutrition (Nini Maine, Functional Nutritionist): We implement a Gastroparesis-Friendly LEKT Protocol. Since GLP-1s slow gastric emptying, standard high-fat keto can cause nausea (“Double Gastroparesis”). We utilize liquid nutrition, MCTs, and texture-modified proteins to hit a target of 1.2g to 1.5g of protein per kg of ideal body weight. This ensures you have the building blocks for tissue repair.
The Training (Danny Trejo, CES): We bring the infrastructure to you—whether in Tarrytown or Downtown Austin. We monitor your recovery metrics. If your grip strength drops (a sign of central nervous system fatigue), we pivot to mobility and fascial release. We operate on the principle of “Minimum Effective Dose” to stimulate retention without inducing burnout.
Comparative Analysis: Standard Diet vs. RxFit Protocol
| Feature | Standard GLP-1 Approach (Caloric Restriction) | RxFit “Asset Protection” (LEKT + Corrective Strength) |
|---|---|---|
| Fuel Source | Glucose (Muscle is burned for fuel). | Ketones (Fat is burned; Muscle is spared). |
| Lean Mass Risk | High (25-40% loss of lean mass). | Low (Protein sparing via $\beta$HB). |
| Metabolic Rate | Drops significantly (Metabolic adaptation). | Preserved (Metabolic engine protected). |
| Training Focus | “Cardio” for calorie burn (Catabolic). | Tension for structural integrity (Anabolic). |
| Digestibility | High risk of bloating/nausea. | Texture-modified for gastroparesis management. |
| Long-Term Outcome | “Skinny Fat” & Rebound Weight Gain. | Body Recomposition & Career Longevity. |
Troubleshooting Side Effects: An If/Then Logic List
Managing the interaction between ketosis, lifting, and GLP-1s requires somatic awareness. Use this logic flow to troubleshoot symptoms.
- IF you experience nausea during training -> THEN switch to liquid protein sources and avoid fibrous vegetables 90 minutes pre-workout (gastric retention).
- IF you feel dizzy upon standing (Orthostatic Hypotension) -> THEN increase sodium intake immediately; ketosis flushes electrolytes.
- IF joint pain feels “sharp” rather than muscular -> THEN stop; rapid weight loss may have exposed structural instability. Schedule an assessment with Danny Trejo.
- IF grip strength or explosive power decreases -> THEN increase daily leucine intake and prioritize sleep; you are under-recovering.
- IF you hit a weight loss stall -> THEN do not cut calories further; increase daily step count (NEAT) to mobilize fatty acids without stressing the CNS.
Conclusion: Protecting the P&L
For the Austin executive, your body is the vehicle for your ambition. The goal of using GLP-1s should not be to become smaller; it should be to become more efficient.
By combining the amino-acid sparing effects of Ketosis with the mechanical tension of Corrective Exercise, RxFit provides a firewall against muscle wasting. We ensure that when you reach your goal weight, you arrive with the strength, posture, and metabolic health required to lead. Stop depreciating the asset. Optimize it.
